
 Background
Background
Levodopa, a pro-drug of dopamine, has been used successfully to treat symptoms of Parkinson’s disease for fifty years and remains the mainstay of medical management. However after years of treatment, with increasing loss of dopaminergic presynaptic terminals, symptomatic control may become more brittle, with sudden and unpredictable “on” and “off” treatment times during the day, or with involuntary movements called dyskinesia. There are theoretical reasons, and some animal model and clinical evidence, why intermittent oral delivery of levodopa may increase susceptibility to these problems through unphysiological wide fluctuations in synaptic dopamine; unfortunately the plasma half life of levodopa after an oral dose is as little as an hour. As a result, other long acting medicines have been introduced, but they may come with other side effects and are simply not as powerful as levodopa.
Relatively steady state levels of levodopa can be achieved by direct intra jejunal delivery. Unfortunately, levodopa is not stable in solution and the gel used to keep levodopa in suspension in a form that can be delivered is very expensive to produce. A year’s treatment in the UK was estimated by NHS England in 2015 to cost around £28000. As a result, despite there being now substantial evidence of the treatment’s effectiveness, there has been a debate about the treatment’s cost effectiveness. Calculations of the cost effectiveness in terms of cost per quality of life adjusted years (QALY) gained vary considerably. The calculations depend not only on the cost of treatment versus standard treatment and the difference in quality of life, but also the carer costs and other costs. So if a treatment is less effective, the patient may be more disabled and cost more. It is unclear, however, how figures on cost of disability can be applied to an estimate of how less effective the treatment is at all points of the severity scale. As far as I am aware there is no actual study showing how much is saved in non medication costs in patients on levodopa-carbidopa intestinal gel (LCIG); the information is instead extrapolated.
In one sense, the QALY gain might be counted twice; once for the intrinsic value of the gain in quality of life, and again for the reduction in disability that resulted in the improved quality of life. In another, this might be a fair way to handle such analysis compared to a treatment that improved quality of life without reducing disability cost.
It is important in such calculations to use reliable data on the magnitude of benefit gained, rather than just to show that there is a gain. This is likely to be achieved by a randomised controlled study with a control arm and is exemplified by the study of Olanow et. al., the subject of this journal club.
Study Design
Sixty six of sixty eight candidate patients underwent the trial. Patients were selected on the basis of having IPD for five or more years, having optimised therapy (meaning a trial of levodopa, a dopamine agonist and one other type of anti-parkinsonian therapy), at least three hours of “off” daily, and no clinically significant psychiatric abnormalities.
At first, assumed that the trial was a cross-over design; in fact it was not. Patients all had jejunostomy procedures but were randomised to LCIG plus placebo oral levodopa, or placebo LCIG plus oral levodopa. They were assessed after a four week stabilisation period before intervention, and then 12 weeks afterwards. Then the two groups were compared.
Patients who were on CR preparations or COMT inhibitors were switched to equivalent immediate release preparations. The LCIG dose was the same as the total daily levodopa dose, delivered over 16 hours of the waking day in the normal fashion for jejunal delivery.
Study Findings
On looking at the graph, labelled figure 2B in the MS, it is immediately obvious that both LCIG patients and oral patients improved very dramatically and then leveled off, despite previously being “optimised” on oral therapy. Our possible suspicions about what “optimised” means are confirmed. As explained by the authors, the doctors had the opportunity to increase the LCIG or oral levodopa during the study, and this was done in a number of cases after the 4 week stabilisation period. In fact the oral medication patients had their medication dose increased more (a mean of 250 mg daily versus 100 mg daily). Despite this, neither group had an increased on time with troublesome dyskinesia.
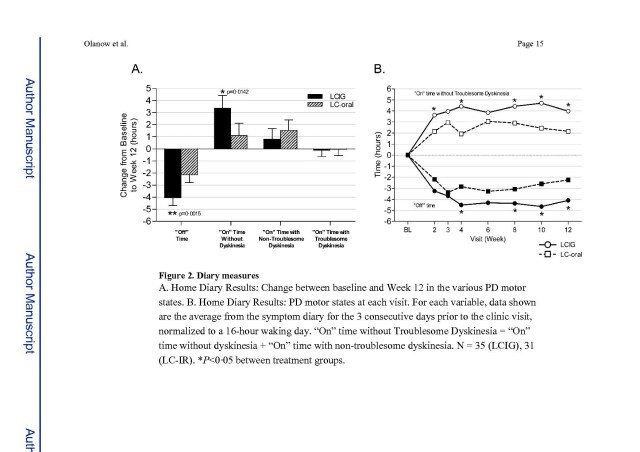
The main message of the study is that after the 12 weeks, the improvement was greater with LCIG, with a mean of around 1.9 less “off” time and 1.8 hours more “on” time without troublesome dyskinesia. I suppose if there is no change in “on” time with dyskinesia, it is obvious that the two values will be similar as one state is replaced by the other.
Regarding quality of life, there was an 11 point versus 4 point improvement in PDQ-39 (a PD quality of life measure. This seems quite important.
Strangely, on the UPDRS there was an improvement in part II (activities of daily living) on LCIG and a worsening on oral, but actually twice as much improvement in part III (motor examination measured in the on state) on oral therapy. Possibly this means that there a subtle side effect of oral therapy, increased during the trial, that adversely affects wellbeing, but the increased “hit” of levodopa made their best on state better than with LCIG.
Comments
It is not clear how the withdrawal of COMT inhibitors made patients in either treatment arm suboptimally treated and therefore needing increased treatment during the study. It would be important to ascertain if by chance the oral arm had had more COMT inhibitors withdrawn.
The main advantage of this study is that having the control arm at least allows us to appreciate that optimised does not really mean optimised. The patients were clearly underdosed; one has to wonder how much better the oral patients could have been if there was the opportunity to optimise them properly by adjusting top up dopamine agonists, adjusting the frequency rather than just the dose quantities and by introducing, reintroducing or optimising COMT inhibition. After all, studies on COMT inhibitors show reduction in on time by about an hour compared to baseline “optimised” therapy.
A parsimonious interpretation of the data is that LCIG simply has better bioavailability than oral; the patients were underdosed and switching to LCIG Is simply stronger and could be replicated by giving more oral treatment. In fact this may well have been the case, explaining the 150 mg more levodopa per day given to oral patients, but the facility for being able to change doses meant its effect would be minimised in this study.
While the power of the study was easily enough to demonstrate a clinically meaningful difference, I wonder if a cross-over design might have allowed intra-patient comparisons and a more clear effect, and eliminated or elucidated the improvement effect from oral therapy. In this design, each patient would have placebo LCIG for half the time, and placebo oral for the other half. The direction of change at the cross over point would be the key parameter. The patients’ doses would be matched at this cross over point, and then not changed over the second half. This design would be confounded by a bioavailability effect, but at least could be measured by the increase in oral dosing during the first half, and there might be an overdose effect of switching from oral to LCIG during the second half of the trial.
Studies looking at the cost effectiveness of LCIG should primarily take data from those like this one, rather than those that use an open label design showing an improvement compared to baseline “optimised” therapy of four hours “off” time reduction. The increased benefit in PDQ shown in this study is nevertheless quite persuasive that there is some real helpful feature of continuous intrajejunal delivery, at least in the short term.
There are other studies that show long term benefits of LCIG but they have not had the same design. Obviously, this design conducted over too long a period would not be ethical; presumably the principle is that all patients after 12 weeks would be offered LCIG, having already had their PEJ tubes inserted. On the other hand, in a longer term study, one would hope that every ongoing effort would be made to optimise therapy in the oral therapy group.
In practice, one must balance benefit versus side effects. Not all patients will want a PEJ tube, or to carry a large cartridge and pump. Virtually all patients had side effects, more serious ones in 13-20%. In 3% the treatment was discontinued as a result of surgical complications, 24% had tube dislocations, 21% insertion complications, 10% stoma complications, 8% pump malfunctions and 7% peritoneal problems. There are reports of neuropathy from LCIG but in this study there were three possible cases in the placebo group and only one in the treatment group.
Finally, LCIG is not the only advanced therapy available. There are no direct comparisons between LCGIG and deep brain stimulation or apomorphine pump therapy to guide as to which treatment to select in individual patients, although the different inclusion and exclusion criteria do provide some help in choosing which therapy is appropriate for which patient. For example, age over 70 and history of depression exclude deep brain stimulation but not LCIG.
