
Background

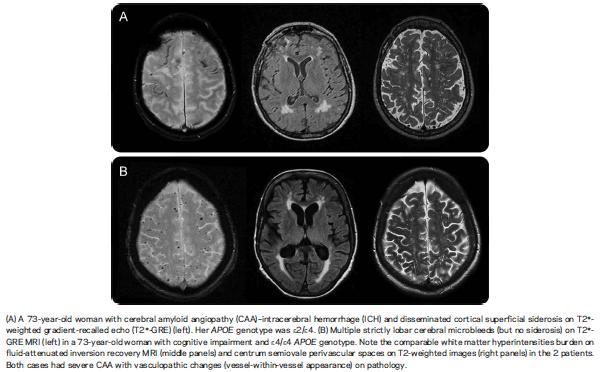
Sporadic cerebral amyloid angiopathy (CAA) is the most common cause of lobar intracranial haemorrhage, which in itself accounts for about 5-10% of all strokes. Amyloid deposition in small arteries of the cerebrum leads to friability and haemorrhage. There are also rare familial forms of amyloidosis affecting the nervous system that more typically result in early onset dementia or peripheral neuropathy, and amyloid deposition in general constitutes part of the pathological process of other neurological conditions such as Alzheimer’s disease.
There is no specific treatment for CAA other than blood pressure control, as hypertension may be an association. It might nevertheless be useful to identify markers of the condition before major symptomatic haemorrhage occurs, so that one can avoid anticoagulants and perhaps antiplatelets in such susceptible individuals.
Potential markers include the apolipoprotein (APO) E ε2 genotype and imaging markers such as superficial siderosis and centrum semiovale white matter perivascular spaces. Superficial siderosis is not specific to CAA, being the result of any cause of chronic cerebral or spinal subarachnoid leakage of blood. Enlarged perivascular spaces could relate to small haemorrhages in the more distant past.
This paper, by Chridimou et al. (2015) in Neurology, looks at these associations retrospectively by a database review of brain biopsies or of evacuated haemorrhage material. These are correlated with MRI findings and APO E ε genotype in patients with positive pathological findings.
Study Design and Findings
The brain biopsy and haemorrhage specimen database review found around 100 cases of pathological cerebral amyloid angiopathy (CAA). Roughly half had had a symptomatic lobar intracranial haemorrhage (ICH). The others were presumably identified coincidentally.
There was no difference in pathological CAA severity between those with or without ICH, but neuritic plaques without neurofibrillary tangles were more likely to be found in ICH cases (53% vs 13%); this is because, as is already known, neurofibrillary tangles are associated with a more Alzheimer type amyloid deposition process. Again as expected, the ε2 allele was more associated with ICH cases and the ε4 allele (a risk factor for Alzheimer’s disease) more likely in the others.
Imaging features of white matter changes, enlarged perivascular spaces and microbleeds were the same in both groups but superficial siderosis was more common in ICH cases (52% vs 20 %).
 Follow up of the non ICH patients 3 years after brain biopsy revealed that 2 of 51 subsequently had lobar ICH; one of these had superficial siderosis changes.
Follow up of the non ICH patients 3 years after brain biopsy revealed that 2 of 51 subsequently had lobar ICH; one of these had superficial siderosis changes.
The study’s main conclusion is that the ICH subgroup of CAA is more likely to have superficial siderosis on imaging.
Strengths and Weaknesses of Study
It is already known that different APO genotypes are associated with Alzheimer’s disease or with ICH, and despite the fact that pathological changes were not worse in the ICH patients it is not surprising that ICH patients are statistically more likely to have the “haemorrhage” genotype than the “dementia” genotype. The presence pathologically of CAA appears to be less specific for ICH as opposed to Alzheimer’s disease than the presence of an APOE ε2 allele or superficial siderosis on imaging.
However, the degree of specificity and sensitivity of these markers is not diagnostically helpful.
The association with superficial siderosis is not surprising as it is a direct marker of haemorrhage more specifically than general markers of small vessel disease that could also reflect atherosclerosis. At least the paper confirms this and raises awareness of superficial siderosis, but anticoagulation would not be given to such patients anyway, even without awareness of the strength of association with ICH. A patient with superficial siderosis would typically be investigated on imaging for a cause of chronic subarachnoid haemorrhage. If no such cause was found, and the patient was relatively elderly, possibly it could be concluded that they were susceptible to CAA and in particular to ICH from such pathology.
Our Journal Club wondered in passing if homozygotes for either ε2 or ε4 had extra susceptibility to haemorrhage or dementia respectively. Certainly, homozygous ε4 carries increased risk of dementia; compared to being homozygous for the “neutral” ε3 allelle, ε4ε4 carries a x15 risk of developing AD, while ε3ε4 carries a x3.2 risk. APOE transports cholesterol and lipoproteins to the neurones by binding to neuronal APOE receptors. Mutations may lead to atherosclerosis because of hyperlipoproteinaemia. The ε2 allele is less efficient at binding so homozygotes may be more susceptible to atherosclerosis. On the other hand one ε2 allele is protective versus the e4 allele in relation to various neurodegenerative conditions including ischaemic stroke!
It is not immediately clear why these polymorphisms of a lipoprotein transporter would influence amyloid deposition into vessels and how friable this would make the vessels become.
A limitation of the study is the selection of patients; it would be heavily skewed to ICH patients because there would be pathology available in many of these. Patients would rarely have a biopsy if superficial siderosis was found on MRI, given its many other causes, and there would presumably have been some other major brain pathology, such as early onset dementia, in the remainder of non ICH cases that would have prompted such an invasive investigation. Hence the increased occurrence of ε4 allele is not surprising.
The true specificity and sensitivity of these markers remains unknown because the biopsy reflects a single snap-shot in time; there may be two subgroups of ICH negative patients, one who have amyloid deposition in blood vessels as part of some other amyloid process, possibly a by-product of dementia-related pathology, and the other who are susceptible to ICH but who simply have not had their haemorrhage yet. Unfortunately 3 years follow up, to see if it is specifically those who also have superficial siderosis who are in the susceptible group, is probably too short to answer this question.
This paper was presented to our Journal Club by Dr Sam Nightingale, Specialist Registrar in Neurology, Queens Hospital, Romford, UK.
