
 Background
Background

One of the main issues facing a patient diagnosed as having had a first epileptic seizure without any sinister underlying lesion – often a young adult and otherwise well – is the driving ban. One can only be sympathetic to the impact that it may have for some on travelling to work or actually performing their job. Some react with understanding, while others have the attitude that they will never expose themselves or others to harm even if the risk is tiny and they later become legally entitled to drive. A few react with incredulity: “I totally lost consciousness without warning, may do so again at any time, and you are ruining my career or social life by preventing me from driving for several months?!”
This can be a difficult conversation for clinicians, but at least one can remind oneself that the conversation might have been more difficult if the cause of their seizure was a brain tumour rather than cryptogenic, in which case they might only be alive for several months.
Two other points can help. First, in the European Union and in most other countries the rules are standardised and set by government authorities. The physician is only explaining the law of the land. In the US, some states have similar standard rules while others, perhaps unfortunately, do leave it to the doctor or to a medical review panel. Second, these rules were developed and modified after extensive review and consultation. Briefly communicating this process may help the patient to appreciate that they are designed to protect, not to punish. The paper reviewed here describes statistical data on risk of seizure recurrence that were used to help develop a consistent European Union Guideline, which informs the UK’s Driving and Vehicle Licencing Agency (DVLA) guideline (2013) and could be used to help doctors who must form their own guidelines.
The paper was published in the good old British Medical Journal (2010) and reanalyses data from the MESS (Multicentre Early Epilepsy and Single Seizure) study (2005), specifically on patients over 16 years of age who had a single unprovoked seizure and looks at the 12-month risk of recurrence at certain time points after the index seizure. In other words, if a patient has already gone some months following an initial seizure without a subsequent seizure, how likely are they to remain seizure-free for another 12 months?
This website had an accompanying commentary that discusses the original MESS study in more detail and the wider issues around prognosis and management after a single seizure. Clearly, the data in this paper are helpful for prognosis, but only in patients who have already gone a certain period seizure-free after their initial event.
Study design
The original MESS study’s inclusion criterion was that both patient and physician were uncertain about whether or not to start antiepileptic medication. Exclusion criteria included previous treatment with antiepileptic drugs or the presence of a progressive neurological disease. Out of around 1800 patients meeting the criteria, 1400 were enrolled; the others refused on the basis that they did not want to be randomised. Demographics showed no particular bias in these patients.
Patients were randomised to immediate treatment – the drug of the physician’s choice as early as possible after seizure (usually carbamazepine or sodium valproate) – or to deferred treatment, generally if the patient had a second seizure.
Where there were around 720 with single seizures in each arm in MESS, in the BMJ reanalysis there were around 320 in each arm who were 16+ and who had had only one seizure at the time of randomisation and whose date of seizure, as opposed to date of randomisation in the MESS study, was known.
Findings
The main finding of the BMJ reanalysis was that in the immediate treatment group the risk of recurrence in the next 12 months, having already gone 6 months without a seizure after the first seizure, was 14% (95% Confidence Interval (CI) 10-18%). In the deferred treatment group the risk rose to 18% (95% CI 13-23%). In the deferred treatment group, if the patient had already gone 12 months without a second seizure, their chance of recurrence dropped to 10% (95% CI 6% to 15%).
The overall general principle regarding driving has been arbitrarily set that if the risk of a seizure is less than 20% over the next year, then it is permissible for the patient to drive a private vehicle and if the risk is less than 2% they may drive a public or heavy goods vehicle. This is not a medical but a policy decision, presumably taking into account the proportion of time that the average person spends driving and the likelihood of risk to self and others should an accident occur as a result. The role of clinicians is simply to provide guidance on which patients have a 20% or greater risk.
It can be clearly seen from the data in this review that if a patient starts treatment, their 12 month risk 6 months after a seizure is lower than 20%. Therefore they may be allowed to drive at 6 months. The same applies to patients not on treatment – if one takes the mean estimate of risk of 18%. However, if a clinician were to be asked, “At what time would you be confident that the risk of recurrence in the next 12 months would be less than 20%”, he or she should use the upper confidence limit for the risk and so the 23% figure for patients not on treatment is too high. Only if patients not on medication have already gone a year without seizures is the upper confidence interval of 15% acceptable.
Strengths and weaknesses of the study
As mentioned in the paper, a potential weakness is that the data were taken from a randomised controlled trial (MESS) of patients having immediate vs. delayed treatment. From looking at the inclusion and exclusion criteria, one might suspect a selection bias that clustered patients of intermediate severity – those who definitely wanted medication or definitely didn’t want medication were excluded. So the risks in the low-risk subcategories might be overestimated and those in the high risk subcategories underestimated.
It could have been a problem that there was an inconvenient delay between seizure and randomisation in MESS of around 3 months. This would rule out patients who had a second seizure in that time. But 3 months is half of the six month seizure free period in which we are interested! Fortunately, in this paper the investigators back-tracked to get the actual seizure time rather than randomisation time; this means that the six month free period is an accurate reflection.
But if one wanted to generalise the findings to prognostication of seizure risk, surely something that the patients will want to know about, if one is making this prognostication on a patient just after their seizure (which should typically be the case as all patients having a seizure should be promptly reviewed by a specialist), then we cannot use the figures from MESS (which included children) or those reviewed here. All we can do is wait three months, say in a subsequent clinic, and if they have not had a seizure in that time, the figures reviewed here can be used. A more full discussion on prediction of risk and decisions on treatment is in the accompanying commentary on management after a first seizure.
Finally, there is the issue of validating seizures in the outpatient department, as was done in the study. Clinicians more inexperienced than those used in MESS might make more mistakes in correctly identifying seizures, or patients might deny or forget seizure occurrences. This is likely to be more of a problem in real life than in a trial. So we cannot say that MESS is overestimating risk, but we can say that MESS does not simulate the real life underestimation of risk that may occur in daily practice.
Different risks in different patients
If the policymakers wanted to finesse the guidelines to take into account other factors, there are adjustments that could be made. In a univariate factor model, it was found that remote symptomatic seizures (seizures occurring as a result of a brain insult e.g. head injury, encephalitis, neurosurgery, that occurred some time before the seizure) were associated with significantly higher risk, as were presence of neurological deficit, seizures while asleep, abnormal electroencephalogram (EEG), and lack of brain imaging information.
Calculating the risks for these subcategories reveals that, if taking the upper confidence intervals, remote symptomatic seizures, neurological deficit, sleeping seizures and abnormal EEG all shift the risk above the 20% threshold after 6 months seizure freedom, and the first two are above the threshold even after 12 months seizure freedom. However, the data numbers are getting small and estimations more inaccurate.
A multivariate analysis of various combinations of factors, much in the same way as risk of osteoporosis can be calculated, is a better way of addressing this issue. This is shown in table 5 of the paper (below), noting that they have excluded patients with a first degree relative with epilepsy and sleep seizures. The latter are a special case; while recurrent seizures are more likely (because they may reflect particular epileptic syndromes) they are also more likely to recur in sleep and so be less relevant for driving risk. The UK DVLA rules now in fact permit driving with continuing sleep seizures provided a pattern of seizures only while asleep has been established for at least 1 year.
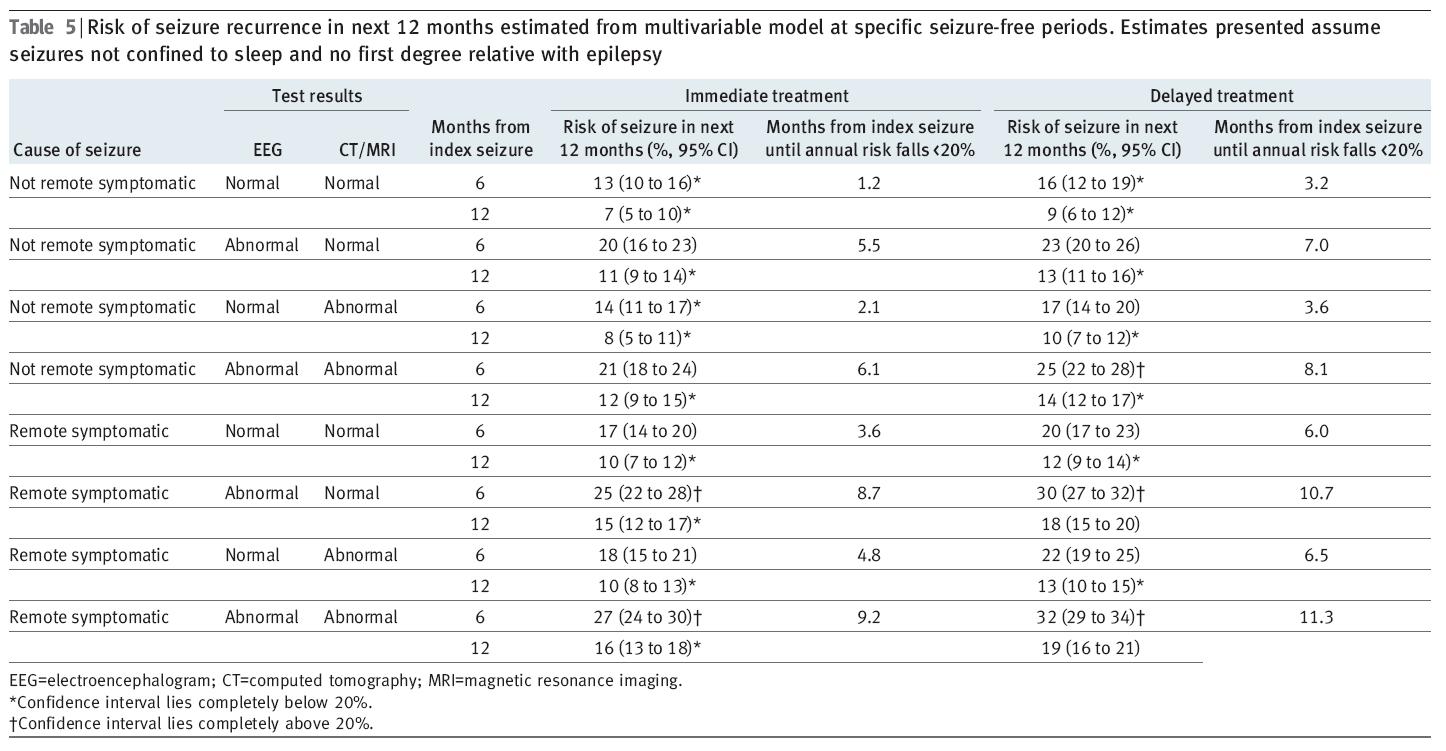
One can see, for example, that a non-remote symptomatic seizure with an abnormal EEG has an upper confidence interval of risk of 23% at 6 months even if imaging is normal. One might argue that the current blanket rule of 6 months is rather lenient for patients with an abnormal EEG or with a remote symptomatic seizure, especially if the patient is not on antiepileptic medication.
A careful view of the wording of the current UK Driving and Vehicle Licensing Agency guidelines in fact includes a clause “provided no risk factors indicate a more than 20% risk of a recurrence over the next 12 months”. If this is interpreted as being confident that the risk not more than 20%, then all the above-mentioned categories would entail a 12 month not 6 month ban, and we would be needing EEGs on everyone to inform this decision. If it is interpreted as being most likely risk level, then abnormal EEG still entails too high a risk if not on medication (23%), as does abnormal imaging if remote symptomatic and not on medication (22%). Only if it is interpreted as being possible that the risk is as low as 20% and the patient was started on medication and the seizure type was non-remote symptomatic is an EEG not necessary because it is only in this circumstance where the lowest confidence interval of risk is not above 20% whether or not the EEG is abnormal.
Data from other studies
A population rather than outpatient based study on 252 patients who had a single seizure as their index seizure (National General Practice Study of Epilepsy (1990)) found a 37% risk of a second seizure within 12 months, and an 18% risk if the patient had already been seizure free for 6 months. This shows just how much the risk level reduces if the patient has already undergone a modest seizure-free period. Factors increasing the risk of recurrence were symptomatic seizures, neurological deficit, and no antiepileptic drug treatment. The findings are therefore comparable to the reviewed data.
Conclusions
This paper clearly does what it intends; to ascertain whether, after 6 or 12 months seizure free following a first seizure, the level of risk of a seizure over the ensuing 12 months is greater or lower than the policy threshold of safe private vehicle driving of 20%.
The analysis provides a rationale for the duration of the driving ban that might help some patients better come to terms with what may seem a punitive measure.
Partly as a result of this study, a number of changes have been made to the UK’s DVLA regulations (2013) regarding epilepsy:
- The ban following a single seizure is reduced to 6 months from 12 months.
- If a pattern of sleeping-only seizures is established for 1 year (formerly 3 years) the individual is allowed to drive.
- If a patient was seizure free on medication, and then a seizure occurred as a result of a medication change, the patient can return to driving after only 6 months if they go back on the original medication.
- If a patient has only ever had seizures that do not affect conscious level or ability to drive, they can drive a year after this diagnosis is established even if they continue to have these seizures.
However, the multivariate analysis of risk factors does raise some issues about higher risk categories, and draws attention to the clause in the DVLA guidelines “provided no risk factors indicate a more than 20% risk of a recurrence over the next 12 months”. I am not sure how many clinicians actually apply this rule.
Could they be sued if a patient had a single remote symptomatic seizure, was started on medication, and had a second seizure 11 months later resulting in a fatal road accident if the clinician had not performed an EEG, or if the EEG was performed and found to be abnormal?
Could they be similarly sued if they had any kind of seizure, but had not started medication and the EEG was not performed or was abnormal, or if both EEG and MRI were abnormal?
Or is there a “get-out argument” that one would have to use the lower confidence estimate of risk to prove that the risk was greater than 20%? In some categories even the lower confidence estimates are above 20%. Happy days for lawyers, if not for everyone else…

Pingback: Journal Club Commentary: Management of Single Seizures | Neurology Online Journal Club